The below videos give a brief description of Servo targeting schemes and ventilator modes that use Servo targeting schemes.
Showing posts with label PAV. Show all posts
Showing posts with label PAV. Show all posts
Tuesday, October 28, 2014
Servo Targeting Schemes
Ventilator modes that use Servo targeting schemes are very responsive and provide the most comfort and synchrony in the spontaneous breathing patient. Servo targeting is "a control system for which the output of the ventilator automatically follows a varying input. This means that the inspiratory pressure is proportional to inspiratory effort" (Chatburn, R.).
The below videos give a brief description of Servo targeting schemes and ventilator modes that use Servo targeting schemes.
The below videos give a brief description of Servo targeting schemes and ventilator modes that use Servo targeting schemes.
Tuesday, November 12, 2013
Incorporating Proportional Assist into Ventilator Protocols
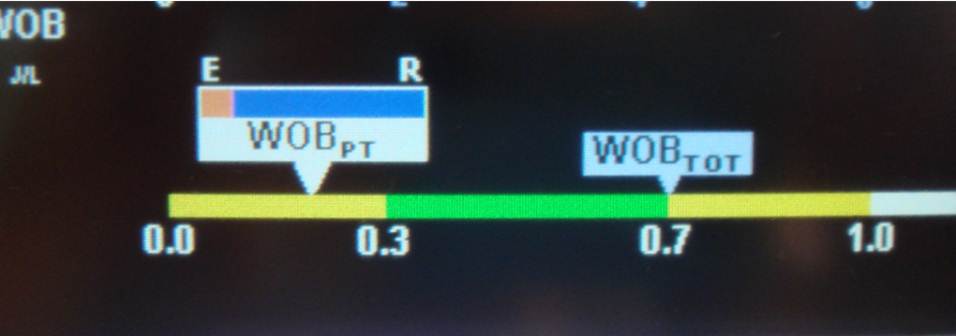 |
| Image 1: PAV+ Work of Breathing bar. |
PAV+ may be used for the initial mode of ventilation during the acute phase of mechanical ventilation. However, from my experience I have had the most success and efficiency with PAV+ utilizing the mode to rest patients after a failed spontaneous breathing trial. After reviewing the literature it is still unclear the best way to wean or liberate a patient from PAV+. However, a traditional T-piece trail has been supported by many peer reviewed journals, so at my institution we still use a 30 minute to one hour T-Piece trial to screen patients for extubation.
How to incorporate PAV+
Monday, February 27, 2012

Monday, November 29, 2010
UTILIZATION OF PROPORTIONAL ASSIST VENTILATION FOR PATIENTS WHO FAIL A SPONTANEOUS BREATHING TRIAL
Background
Unloading ventilatory muscles has been a primary issue with our ventilator population. After analyzing ninety samples, it was revealed that 81% of the failed spontaneous breathing trials (SBT) were related to rapid, shallow breathing. Our original process for resting patients who have failed a SBT was to ventilate the patient utilizing “Volume Control Ventilation plus” (VCV+). One disadvantage of using an assisted mode for resting patients is the inability to properly set the ventilator to provide adequate rest without over resting the ventilatory muscles. Another disadvantage is patient/ventilator asynchrony, which may occur at any phase of breath delivery. A study of “Proportional Assist Ventilation” (PAV) was initiated to explore potential advantages over VCV+.
Unloading ventilatory muscles has been a primary issue with our ventilator population. After analyzing ninety samples, it was revealed that 81% of the failed spontaneous breathing trials (SBT) were related to rapid, shallow breathing. Our original process for resting patients who have failed a SBT was to ventilate the patient utilizing “Volume Control Ventilation plus” (VCV+). One disadvantage of using an assisted mode for resting patients is the inability to properly set the ventilator to provide adequate rest without over resting the ventilatory muscles. Another disadvantage is patient/ventilator asynchrony, which may occur at any phase of breath delivery. A study of “Proportional Assist Ventilation” (PAV) was initiated to explore potential advantages over VCV+.
Friday, November 5, 2010
THE APPLICATION OF PROPORTIONAL ASSIST VENTILATION IN A PATIENT WITH DECOMPENSATED CONGESTIVE HEART FAILURE
Introduction
In patients who failed wean criteria, our standard of ventilator management utilized PC-CMV. However, it is well-known that positive pressure ventilation can profoundly alter cardiovascular function.
Admitted to our ICU was an 85 y/o male with an extensive cardiac history significant for Sick Sinus Syndrome, Paroxysmal Atrial Fibrillation, and Atherosclerotic Coronary Artery Disease, with an estimated Left Ventricular ejection fraction of 25%. The patient’s surgical history was significant for pacemaker placement and percutaneous coronary intervention. On ventilator day 3, the patient’s ventilator mode was changed from PC-CMV to Proportional Assist Ventilation (PAV) to allow for unhindered spontaneous breathing in an effort to increase cardiac output (C.O.)/index (C.I.).
Case Summary
The patient was intubated due to hypoxic ventilatory failure secondary to decompensated congestive heart failure. Immediately following the application of mechanical ventilation, the hypoxemia was reversed, yet the cardiac instability persisted and prevented the patient from progressing to spontaneous breathing trials. Initial ventilator settings were PC-CMV, Vt 450, RR 14, FiO2 30%, & PEEP of 5. Respiratory and hemodynamic measurements were obtained before switching the mode to PAV, 80% support, FiO2 30%, & PEEP of 5 and the patient was allowed one hour to stabilize after modality change before obtaining an additional set of parameters. Pharmacological agents included a Dobutamine infusion @ 4mcg/min and a Propofol infusion @ 5cc/hr. No pharmacological changes were completed during data collection or alternating between ventilator modes.
Our patient’s initial C.O. on PC-CMV was 3.06 L/Min with a C.I. of 1.56 L/Min/M2. Upon conversion to PAV, the patient’s C.O. & C.I. increased by ~27% while the PaO2 increased by ~17% (Table 1). After observing hemodynamic improvement with PAV, the patient was maintained on PAV and the Propofol infusion was rapidly terminated. On ventilator day six, the Dobutamine infusion was discontinued and the patient was extubated without complication.
Discussion
In our patient PAV produced a higher C.O. & C.I. over PC-CMV which is similar to the results Kondili documented when comparing PAV to pressure-support ventilation. Conversely, spontaneous variability of C.O. should be considered when evaluating two measurements taken at separate times. Sasse revealed that variability of C.O. may differ as much as 10%. 1. Proportional Assist Ventilation: Guidelines for Using PAV+
Subscribe to:
Posts (Atom)